Five Questions
Good morning!
It’s the last Friday of the month so today I’ll answer your questions.
Just as a reminder, I appreciate all of your questions and comments and read all of them. I can only answer a limited number in this space, but I pass the rest along to senior administrators for review and possible action.
Now, let’s go to your questions.
Q: What happened to the power washing of buildings? This made a big difference on the critical care tower. I think the appearance of the hospital, both outside and inside, makes a difference in how patients and families perceive the hospital as a whole.
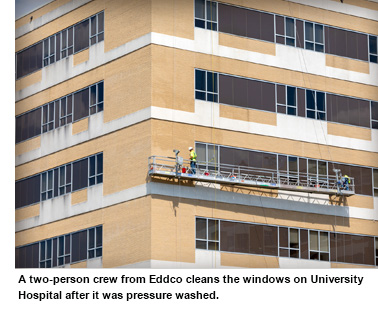 A: I couldn’t agree with you more about the positive impression a clean building makes, not only outside, but inside. Each time I make walk rounds (and I try to do this most days) I pick up paper and trash. I encourage all of you do to the same to help keep our campus environment as clean as possible. About a year ago the exterior appearance of our buildings concerned me, so I asked our administrative services team to work on it. They determined that we have nearly 207,000 square feet of exterior surface on buildings that should receive either quarterly, bi-annual or annual pressure washing. We are able to wash some of these structures ourselves; others require specialized equipment and that work has to be contracted to an outside vendor. We have a power washing project ongoing at almost all times. A vendor began pressure washing University Hospital right after Labor Day. Depending on the weather, that process will take about three months. The cost to clean one of our larger buildings can range in the hundreds of thousands of dollars. Our Facilities Services team will be tackling some smaller projects after they winterize our lawns and flower beds.
A: I couldn’t agree with you more about the positive impression a clean building makes, not only outside, but inside. Each time I make walk rounds (and I try to do this most days) I pick up paper and trash. I encourage all of you do to the same to help keep our campus environment as clean as possible. About a year ago the exterior appearance of our buildings concerned me, so I asked our administrative services team to work on it. They determined that we have nearly 207,000 square feet of exterior surface on buildings that should receive either quarterly, bi-annual or annual pressure washing. We are able to wash some of these structures ourselves; others require specialized equipment and that work has to be contracted to an outside vendor. We have a power washing project ongoing at almost all times. A vendor began pressure washing University Hospital right after Labor Day. Depending on the weather, that process will take about three months. The cost to clean one of our larger buildings can range in the hundreds of thousands of dollars. Our Facilities Services team will be tackling some smaller projects after they winterize our lawns and flower beds.
Q: DIS offers many training courses in the Technology Learning Center (TLC). I would like to participate in some of them, however, they are only offered during the times that I am doing patient care. Why are they not being offered on the weekends/evenings when others can potentially participate in them?
A: I posed this question to leaders in DIS. Their response: In the past, DIS offered classes after hours for those providing patient care during normal business hours. However, these classes were sparsely attended. The team has decided to create eLearning opportunities for on-demand training. These course offerings will mirror what the TLC offers face to face and will be loaded in our HealthStream catalog. The goal is to have some of these courses available by the end of October. Be on the lookout for communication as these become available to the organization. Thank you for your interest and for this question. We need to do all we can to be sure our learning opportunities are widely available.
Q: I would like to see if we can get drug samples brought back to our outpatient clinics. This new policy has really caused a hardship on our patients who have bad or no drug insurance coverage. There are many medications that are too expensive for some of our patients who rely on these samples. Also, our doctors often want to start a patient on samples for a new medication to see how the patient tolerates it prior to making the patient have to purchase an expensive medication or having to get it approved by their insurance company. Doing away with samples in all of our outpatient clinics has really decreased our quality of service and patient care. I really don't know why samples were discontinued in the first place. Can we please get medication samples back in our clinics?
A: My understanding is that the policy you reference restricting the use of drug samples in the ambulatory clinics was implemented in July. This practice was already in place in our hospital-based clinics. Our actions are in line with those of other academic medical centers nationally to remove drug samples from the outpatient setting. There are a host of reasons to do this, but the most important are the inconsistencies in the use of samples with regard to safety practices, storage, labeling and dispensing standards. When samples were prevalent, it was not uncommon to find large quantities of expired medications, a lack of appropriate record-keeping and non-compliance with product recalls. It was also widely recognized, here and elsewhere, that the provision of drug samples by pharmaceutical companies had become a means by which industry representatives gained unfettered access to clinics and medical staff to potentially influence prescribing practices. Even though the new policy largely restricts the use of sample medications in the clinic setting, requests for exceptions are considered, first by the respective department chair and then by the full Council of Clinical Chairs. While I recognize that many patients, and especially our lower-income patients, benefitted from the availability of samples, avenues remain for patients to receive reduced pricing on their medications through our participation in the federal 340B program and through coupons, vouchers and financial assistance provided by manufacturers.
Q: This question is in regard to the PGA Golf tournament. Why is it that we have to use personal leave time to volunteer during the week and not given at least four hours of administrative leave?
A: First, I want to thank all of you who volunteered at last week’s tournament, and especially those who took personal leave to work during a weekday. More UMMC staff – 176! – volunteered this year than at any previous tournament, and I’m proud of that. With regard to your question, while the Sanderson Farms Championship directly benefits our children’s programs, there are many wonderful groups and activities that also directly or indirectly benefit the Medical Center or do things that are also helpful to us. Even if we could pick and choose between these worthy activities to award time off to our staff for serving as volunteers, we do not have the authority to do that.
Q: Could you address the problem with the broken set of C elevators in the adult hospital? It has been months since they have worked. It really has been an inconvenience and a burden to have two out of four main elevators not functioning.
A: Our Facilities Services staff report that we began having problems with Elevators 3 and 4 last spring. The elevators are original to the adult hospital and the motors and hoist cables on both were in need of replacement. As I’m sure you can imagine, replacing components on 64-year-old elevators is no small undertaking, both logistically and from the standpoint of expense. Rebuilding the motor alone costs $100,000 and has to be done on site. We do have a projected return-to-service date for Elevator 3 of Nov. 1. Work will then shift to Elevator 4 and should take a minimum of four weeks. In the meantime, I apologize for the inconvenience.
Keeping up with all the needs of our growing academic medical center is a tall order, and we appreciate all that it takes to keep this place operating at full throttle, in our quest to achieve A Healthier Mississippi.