Pain led John and Linda Cook on a fearful, frustrating journey that started in a hospital emergency room and ended in a 12-hour surgery at the University of Mississippi Medical Center.
Cook said he gave in to abdominal pain the third time it struck, seeking help in his Columbus hometown.
What doctors found confounded them. Multiple tumors and mucous filled his belly, obviously the cause of the pain.
“They told me 'We don't know what that is and don't know how to deal with it,'” Cook recalled.
His medical condition is rare, said Dr. Shannon Orr, assistant professor of surgical oncology in the UMMC Division of Transplant Surgery, who saw similar cases during his fellowship at M.D. Anderson Cancer Center.
The weight gain and pain came from tumors growing in his abdomen, attached to the peritoneum, a membrane that lines the abdominal cavity. Over months those tumors grew, secreting a thick mucous and filling his belly.
When he arrived at UMMC, Dr. Kirsten Gambrell, then chief resident for surgery and now a fellow in surgical critical care, realized he might be a candidate for a unique surgery.
On May 12, Cook became the first patient at UMMC to undergo cytoreductive surgery and hyperthermic intraperitoneal chemotherapy or HIPEC, a fancy name for a process in which Orr, Gambrell and a team of others remove the tumors and mucous, any other malignant tissue they find, then flood his abdominal cavity with a heated saline and chemotherapy solution to destroy any remaining cancer cells.
“We take out everything, give him the chemo, then put him back together again,” Orr said. “That way, there's no closings or sutures for tumor cells to hide behind.”
It probably started with appendix cancer, said Orr, who led the surgical team. “About nine months before he presented, he remembered having a lower right quadrant pain and fever. His appendix most likely ruptured because of the cancer.”
But Cook didn't go to the hospital then. When the pain subsided, he figured he'd had a virus or food poisoning. A few months later after eating out with his brother in law, he again experienced abdominal pain. Again, he blamed it on food poisoning.
Tumor cells spread, grew and secreted mucous.
“His belly was huge,” said his wife, Linda Cook. “I thought it was from the beer. He'd have one or two at night. My sister was the first one who said to me, 'I think John has a tumor.' ”
Those words came just days before his April ER visit provided the proof. Pain medication and a biopsy followed.
“They stuck a needle in my abdomen,” Cook said. “When they pulled that thing out and put it in a petri dish it looked like fish eggs, like those pellets you put in the soil to keep it moist.”
Soon Cook became part of a medical referral network Mississippi doctors have been working to build. He was referred from Columbus to specialists at UMMC.
“Everybody was interested in it because it was so unusual,” Linda Cook said of their initial UMMC visit. “The first doctor, Dr. Gambrell, she explained everything so well to us.”
In this type of cancer, mucinous adenocarcinoma, if the appendix bursts, the tumor cells may float in the belly, attach to other organs and start growing. Orr said chemotherapy delivered through the blood supply doesn't work as well since the tumors are tenuously connected to a blood supply.
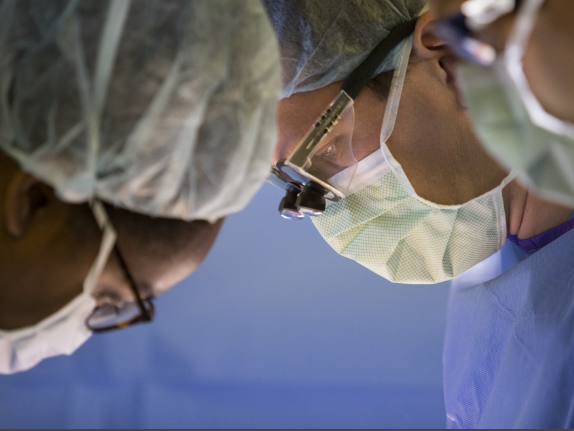
Dr. Kirsten Gambrell, left, and Orr work to remove tumors from Cook's abdomen.
Gambrell said she reviewed the images sent from Columbus, got a few more and then studied them with the radiologist. “We went through the scans and sure enough, he agreed it was probably appendiceal mucinous adenocarcinoma.”
About a year earlier, she had presented a Grand Rounds, a surgical session where doctors go over different procedures, on the HIPEC procedure.
She messaged Orr, “I think we've got someone with a mucinous producing mass.”
Keeping the Cook family informed was a priority, she said. “Families can be confused and upset in these situations but they were very patient and understanding and allowed us to do our jobs.”
Linda Cook said she found relief in knowledge. “She explained everything so well to us,” she said of Gambrell.
A few days later, Orr discussed the surgery and apologized for a two-week delay in arranging to get equipment needed for it. “That didn't bother me,” Cook said. “No one else had given me a chance.”
It's a long and intensive surgery, Orr said. “We probably filled five buckets, gallon buckets, with mucous and tumors. I'd guess it was 20 pounds or more.”
I had done similar surgeries in fellowship at M.D. Anderson, but it was the first one here and in Mississippi,” he said.
Orr said the surgery is right for only a few people. Those might be folks like Cook, who had an appendix cancer, or more likely someone who had colon, rectal, ovarian and some types of gastric cancers with tumors developing in their abdominal cavity.
If cancer has spread beyond the abdominal cavity, this surgery likely will not help. Orr said patients with peritoneal carcinomatosis without distant metastatic disease, should be evaluated for HIPEC.
“As we learn more about tumor biology, we realize there is a subset of people who are going to develop lung metastasis or liver metastasis and this is not going to help them,” Orr said. “And there's a subset that is going to develop peritoneal metastasis and this may help them.”
Doctors use computed tomography scans to find the tumors. If tumors have grown around the ureter or the blood vessels to the liver, the procedure is unlikely to help.
The types of chemotherapy available are limited. A drug that works by being ingested, for example, wouldn't work in this scenario, Orr said. Usually it's either cisplatin, often used to treat bladder, ovarian or testicular cancers, or mitomycin C, often used to treat pancreatic or gastric cancers.
“It's a one-time thing in the OR. The dosage is based on body surface area,” Orr said. “We surgically remove anything with tumor on it. That's the main operation.”
Then they place cannulas, tubes through which the saline and chemotherapy can flow, as well as temperature probes into the abdomen. Once they had sewn the abdomen shut, Orr and Gambrell then infused the heated solution and gently agitated it in Cook's abdomen for about 90 minutes to ensure the chemotherapy hit every available surface. The therapy allows doctors to use stronger chemo doses than those given in an IV and the heat helps the chemo better penetrate cancer cells, Orr said.
After draining the solution, the duo surgically repaired Cook's diaphragm and other areas and closed.
Orr calls Cook the “ideal first patient.” He was healthy, except for the cancer, and had no other life-limiting conditions such as heart problems or COPD.
This will never be a common surgery, said Orr, who now has performed two here. And, it likely will not be one done outside an academic medical center or larger cancer center, Orr said.
“This is among the surgeries UMMC needs to offer if we are to be a center that provides complex care for people with rare conditions.”
Having the option here will allow patients to get treatment they need closer to home. That makes it less expensive, less emotionally draining and allows them to stay closer to their support network.
That was important to this family. “When they told me it was cancer, it never really registered,” Cook said. “I'd never been sick in my life.”
Linda Cook agrees. “It's very overwhelming. I was standing at Starbucks when Dr. Orr came out of surgery. I was staring and he was so happy and so tired.”

John and Linda Cook
It's a type of surgery that requires assistance from many others with multiple talents and it's great for residents to observe, Orr said. “They get to see something they don't get to see every day,” he said.
Recently, a trio got to see something every doctor wants to see.
Two residents and a medical student followed Orr as he entered a clinic room where the Cooks waited for results of a follow up CT. “All clear?” Cook asked. Grinning, his hands in his lab coat pockets and rocking slightly, Orr responded, “All clear.”
Cook, a lanky man, who leans toward blue jeans and cowboy boots, said, “I just had a feeling everything was OK. I feel like I'm getting stronger.”
Now the couple, married 24 years, can focus on life in retirement, or in Cook's case, learning another new skill.
He's worked in construction, in retail and captained an offshore boat. Now, he hopes to learn to repair guns and become an even bigger history buff.
He advises others who must undergo extensive surgeries, “Keep a good attitude and hope for the best; trust your doctor.”
Recovery was painful, he said, adding he clung to one of his wife's favorite sayings, “This too shall pass.”
And, this surgery? “I wouldn't recommend it as a weight loss method,” he said, estimating he lost about 50 pounds in the process, including the estimated 20 pounds doctors removed in surgery.
He has one final piece of advice: “If you have tremendous pain in your abdomen, get it checked out. Don't try to self-diagnose.”
Photos